The Covid-19 pandemics have exacerbated the double burden of malnutrition (DBMN) among mothers and children in low-and-middle-income countries (LMICs). There are several challenges faced by the government to reduce the DBMN in the Covid-19 pandemic era: 1) limited framework for governing and integrating existing policy interventions among G20 countries; 2) competing budgetary priorities and ineffective checks-and-balances system for DBMN interventions; 3) designing more accountable and effective delivery of social assistance in the form of nutritious foods & supplement packages. In this policy brief, we advanced four proposals: 1) Operation of a G20 DBMN alleviation action team; 2) Provide nutritious foods and supplement packages based on defined eligibility criteria and centralized data; and integrate mandatory nutritional education for recipients; 3) Create a framework of collaboration for private sectors, local communities, and international organizations; and 4) empower T20 to be the center of strategic analysis.
Challenge
The Covid-19 pandemic is predicted to aggravate the double burden of malnutrition (DBMN) worldwide, especially in Low-Middle Income Countries (LMICs). The pre-pandemic data and analysis on DBMN have shown that it is already difficult for the world to reach Sustainable Development Goal 2 – ending hunger and all forms of malnutrition, even without the added impact of the pandemic (UNICEF, 2020).
The World Obesity Atlas 2022 (World Obesity Federation, 2022) reports the hike in obesity trend in G20 countries such as The United States, Canada, Turkey, Australia, India, and Indonesia. At the same time, India, Indonesia, and most LMICs are pressured to combat undernutrition prevalence despite already making some progress. DBMN is a “silent epidemic” that will affect not only the health of people globally but also productivity rates, thus requiring immediate solutions.
Several pieces of literature highlight how health/biological, environmental, and socioeconomic factors contribute to the prevalence of DBMN both in developed & developing countries (WHO, 2017). In response, many countries have been stretching the effort to address nutritional issues, sanitation, poverty, lifestyle, or even social and environmental problems. As a result, multiple policy interventions/approaches are being adopted, which require more significant financial support, collaboration across stakeholders, and better monitoring mechanisms (Jacob et al., 2019).
The significant difficulty that countries must face from the approach above is to ensure that each policy intervention is profoundly relevant to solving the nutritional problems and be delivered to the accurate recipients and areas with effective budget spending. When a policy is derived from global commitment, the policy implementation must also consider country-specific context with thorough monitoring and evaluation scheme involving systematic capacity planning with leaders’ commitment as the underlying.
Since WHO introduced the double duty actions “DDA” for combating DBMN in 2017, the policy interventions can no longer be seen as one fit for all. Countries are expected to carefully assess and design more integrated policy interventions to address the DBMN problems simultaneously. Therefore, combining the existing policy interventions with better governance efforts can be the key to helping combat DBMN in times of crisis.
Additionally, the number of both undernutrition and overnutrition are likely to worsen due to obstruction in basic and essential health services as well as food and nutritional supplementation delivery since the start of the pandemic (Headey & Ruel, 2020). If untreated, a study estimate that an additional US$1.2 billion per annum will be required to mitigate the impacts of COVID-19 on maternal and child undernutrition globally (Osendarp et al., 2021).
With ascending financial pressure alongside competing budgetary priorities, evidence-based recommendations and tailored policy designs on efficiently spending public health resources are essential. Therefore, the G20 must play its role in helping these countries achieve sets of common goals through an application framework and implementing “quick wins” in a more accountable manner.
Proposal
Operation of a G20 DBMN alleciation action team
In October 2021, G20 countries agreed to establish a task force to coordinate global collaborative measures and mobilize mutual funds for better pandemic and future health emergencies preparedness. This task force is called Joint Health and Finance Task Force (JHFTF). This task force has moved the discussion towards equality of vaccine distribution, the removal of trade barriers, global food security, and many aspects related to pandemic preparedness (Jessica, 2022). On the other hand, the issue of DBMN is worsening and possesses a greater risk of health in the future, but is yet to be discussed by this task force. Hence we propose to advance the discussion of DBMN alleviation and create a DBMN alleviation action team under JHFTF.
The rationale behind DBMN being the mutual issue that must be addressed through JHFTF is because, first, DBMN issues are veritably a hidden crisis that must be tackled together. While LMICs face problems of coexistence of under- and over-nutrition, high-income countries (HICs) face obesity among poorer households (Perez-Escamilla et al., 2018) which will result in an irreversible economic downturn and health impacts in the long term. Secondly, G20 countries represent two-thirds of the world’s total population or about 85% of global GDP, indicating how strategic the G20 position is to drive the DBMN resolution. Thirdly, the world is facing financial constraints, so adequate health financing, including delivering basic and essential services, must remain a priority. G20 JHFTF shall be able to be the hub for synchronized action, providing an opportunity to exchange strategy and knowledge, global monitoring of progress, and enhanced and equalized institutional capacity to carry out the DBMN alleviation strategy through high-mobilization of the fund and human resources.
The DBMN alleviation action team is responsible for orchestrating the G20 global program for combatting DBMN, starting from designing an intervention strategy, the financial coordination to manage DBMN alleviation funds, and developing a framework of collaboration. Therefore, this team shall consist of relevant stakeholders, including scientists, experts, relevant ministries, international organizations, independent audit agencies, and local community representatives. The framework consists of priority agendas and deliverables elaborated in the below diagram:
Graph 1: The DBMN Alleviation Intervention Cycle
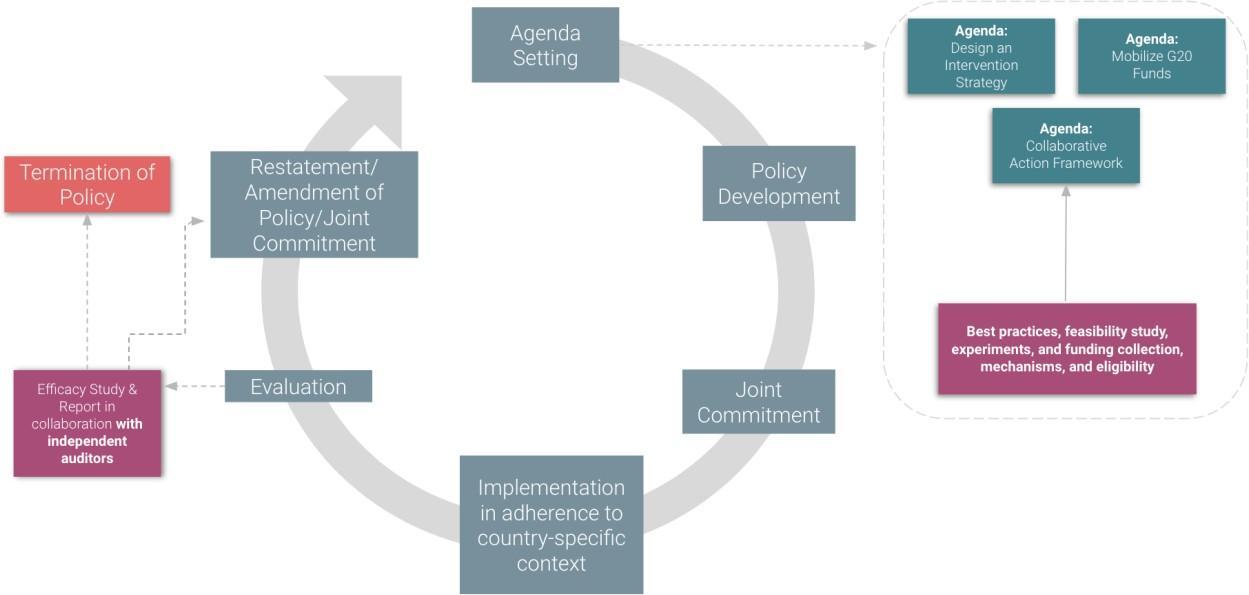
Source: Adapted from National Audit Office United Kingdom (2008)
The above framework portrays how policy intervention is carried out. The type of intervention might be different from one country to another, but the framework provides standardized guidance for designing an accountable, feasible, and sustainable strategy. The first is agenda-setting. There are three general agendas that should be present in each cycle:
1) designing the intervention strategy (element of action);
2) mobilizing G20 funds (element of funding);
3) collaborative action framework (element of stakeholders).
The design of intervention strategy should be done by sharing the best practices from the successful countries; insights-gathering from different stakeholders, such as international organizations, private sectors, and local communities; and conducting experiments and research by experts and scientists (e.g.: randomized-controlled trials) to ensure the workability of the intervention in the targeted area. Meanwhile, mobilizing G20 funds should aim to collect and distribute the funds to support the intervention. The critical part of this agenda is to create a set of criteria for the eligibility of the fund recipient. Hence, the independent auditors should also be present in this stage to assess the fairness of the fund distribution scheme. Lastly, developing a collaborative action framework is the agenda’s aim to specify the roles and expected contributions from different stakeholders that will be elaborated on further in the third proposal.
After designing an intervention strategy, the next step is to develop a policy that can be applied nationwide. Then, to strengthen the collaboration, there should be a joint commitment signed by the representatives of G20 countries to mark the start of implementation. At the implementation stage, the intervention is expected to work. Even though it has been planned thoroughly, the chance of the intervention to be failed still exists. Hence, the evaluation of implementation should be carried out carefully by independent auditors, for example, by conducting an efficacy study. The result of the evaluation can be restatement (where the intervention works and should be continued), amendment (where the intervention can still be continued but needs revision), and termination (where the intervention does not work as intended and needs to be replaced by the new strategy). The cycle goes back to the agenda-setting at the start of the year.
Provide nutritious foods and supplement package based on defined eligibility criteria and centralized data; and integrate mandatory nutritional education for recipients
Social protection plays a pivotal role, especially for vulnerable groups such as mothers and children until the age of 5. As part of pandemic responses, governments worldwide have carried out social protection through various schemes such as cash and basic food transfers, social insurance, tax-funded social benefits, pension coverage, and other feasible mechanisms for guaranteeing basic income security and sustenance (Grosh et al., 2022).
As DBMN cases worldwide are projected to rise, we propose that governments adopt social protection schemes to prioritize nutrition-specific intervention1 for undernourished mothers and children through nutritional supplementation and food. A study has shown that a one-dollar increase in a per-capita nutrition-specific intervention in countries with the highest burden of malnutrition is associated with sharper reductions in the proportion of stunted children (Khalid et al., 2019). The package distribution should be done robustly and accurately by utilizing centralized data gathered by the government with the help of communities and other stakeholders. Nutritious food and supplement packages shall include vitamins, baby porridge, baby milk, and supplements for pregnant women and new mothers on top of basic/staple foods.
1 Nutrition-specific intervention can be defined as interventions that address the immediate determinants of fetal and child nutrition and development (Khalid et al., 2019)
There are three major determinants for implementing this intervention as part of covid- 19 responses;
First, the government must define the eligibility of beneficiaries
The priority of recipients should start from low-income families. Hence, countries must set the eligibility criteria that can be based on monthly income, number of children within a family, individuals’ participation in previous or existing social protection programs, and other sets of criteria as the prerequisite for receiving this aid. The eligibility criteria must be backed by comprehensive analysis and reviewed periodically, where the expansion of beneficiaries’ coverage should be conducted gradually based on the government’s capacity.
Second, the government must implement data collection of the targeted vulnerable groups stored in a single database with the help of grassroots communities and local governments
Central government must work together with local governments and grassroots communities to collect precise data of beneficiaries where details such as name, age, locations, socioeconomic status and conditions, and nutritional intake record of beneficiaries obtained first (either manually or digitally) stored in one database which can be referred and accessed by central and local governments. The central government can apply incentives for participating local government or grassroots communities in the form of recognition or financial reward for boosting their motivation and accountability (which will be elaborated on further in the next recommendation).
These collected data will not only help the central government to estimate the cost of spending but also in deciding the types of foods that are needed for fulfilling the dietary needs of targeted beneficiaries for preventing or treating DBMN. Countries such as the UK, Philippines, US, and Chile have highlighted the importance of animal-based protein such as cow’s milk, fish, and eggs in early childhood as well as micronutrients such as iron, zinc, folic acid, and other multivitamins during pregnancy (NHS, n.d.).
Third, design a system that includes a mandatory education about nutrition as the prerequisite of receiving the package
The local government can utilize existing community-based centers and religious places to communicate the program along with the education about standard nutrition for children and mothers with the help of doctors, pediatricians, and/or dieticians who will be assigned at those centers. To step up the program, socialization can be made mandatory before receiving the package.
Following the mission to spread as much awareness, the socialization can utilize a mobile nutrition center (with possible collaboration with private sectors) to reach rural areas where recipients can redeem their vouchers and card, learn about stunting, nutrition, and dietary guidelines, as well as consult about their medical conditions.
Governments can also collaborate strategically with private providers such as pharmacies, retail outlets, and e-commerce platforms as official distribution channels for the package, particularly for poor families living in urban or suburban areas. This will allow the targeted recipients to obtain packages quickly and allow the government to explore suitable mechanisms. For example, vouchers/voucher codes might be preferred for this type of collaboration where recipients can just go to the nearest pharmacies, supermarkets, retail outlets, or through e-commerce platforms to exchange their vouchers or voucher codes for a bundle of supplement packages. The government could reimburse the payment to private partners based on the transaction, which will boost the check-balances system.
Create a framework of collaboration for private sectors, local communities, and international organizations
The next recommendation is to develop a framework and suitable incentives that can endorse collaborations between stakeholders. The area of collaboration includes funding and execution. At least three key players are expected to join hands with the government. Each player has a different segment of contribution and roles. See the difference in the table below.
| Aspect | Private Sectors | International Organizations | Local Communities |
| Major collaboration |
|
|
|
| Stage of collaboration |
|
|
|
| Type of incentives |
|
|
|
Private sectors. Private sectors consist of companies and corporations with both local and international scopes committed to contributing to the DBMN alleviation plans. The primary collaboration expected from the private sector is in the form of funding and the provision of facilities and human resources. The funding should be delivered to JHFTF and pass the assessment of funding to be free from any potential conflicts of interest and legal consequences.
Aside from funding, the contribution can also be in the form of facilities, infrastructures, and human resources that can support the municipal government’s capacity to carry out the intervention. This kind of support has already been implemented in the Covid-19 pandemic alleviation. Corporates and organizations across the world join hands with the municipal and regional governments to distribute vaccines by opening up vaccine booths and lending their cars or spaces to treat Covid-19 patients (USAID, 2022). In terms of the timing of collaboration, the private sector can contribute in the policy development stage where their insights matter for the design of policy and ensure their share of contribution is captured at the right expectation.
Meanwhile, regarding participation, the motivation of the private sector to join this program might consist of intrinsic and extrinsic motivation. The intrinsic motivation can be from the warm-glow feeling after helping others or the personal satisfaction in carrying out the social cause.
Meanwhile, extrinsic motivation can be in the form of tangible benefit they reap from participation. Intrinsic motivation might exist and influence the participation of private sectors, but we can only control the incentives that trigger extrinsic motivation. In regards to that, we recommend that every corporate or private player that contributes to the intervention receives proper recognition from the government. This can be in the form of a) a certificate or the stamp put in their annual report indicating that the company is recognized as the partner of G20 DBMN alleviation intervention; and b) a display of recognition on the website of G20 or JHFTF. These incentives aim to trigger a reputational effect. According to Bebbington et al. (2008), corporations that disclose and are recognized for their social impact gain an increase in reputation among their stakeholders and investors.
International organizations. International organizations are organizations, including NGOs, oversee the issues of DBMN and willingly contribute to the mission. The significant contribution expected from their expertise is to design social campaigns and socialization strategies, especially because the target of this intervention is mainly from the grass-root level. International organizations are also expected to be the watchdog of the intervention implementation and might collaborate with independent auditors to provide recommendations.
The contribution of international organizations is in these three stages: 1) policy development (sharing of knowledge and expertise); 2) implementation (grass-root campaign); and 3) evaluation. The appropriate incentives might come from the recognition from the government and project funds from the donors to carry out their part in this plan.
Local communities. Local communities include local movements, local youth organizations, mother-and-children advocacy groups, and the group of people with DBMN alleviation-related visions. These local communities come from the targeted; hence, they understand the local context the best, especially regarding the approach strategy. Hence their insights will be valuable in the policy development stage, and their expertise will be useful in the implementation. Aside from acknowledgment, financial incentives should also be considered as this intervention might take their time and resources. Hence, they should as well be properly compensated.
Empower T20 to be the centre of strategic analysis
The last recommendation is to utilize T20 as the think tank group that equips every decision of funding and intervention with evidence-based analysis. We recommend three critical roles for T20 to be involved in the process cycle of the DBMN alleviation strategy. These roles are 1) to analyze and develop eligibility criteria for funding recipients (e.g., countries or organizations) to participate in DBMN Alleviation Intervention; 2) to conduct a pilot project, experiments, research, and feasibility study for determining the most suitable intervention (ex-ante); and 3) to monitor, evaluate, and do efficacy study of the ongoing intervention together with independent auditors, in advance of providing strategic recommendations, whether the interventions should be continued, improved, or terminated (ex-post).
References
Bebbington, J., Larrinaga, C., & Moneva, J. M. (2008). Corporate social reporting and reputation risk management. Accounting, Auditing & Accountability Journal, Vol. 21(3), pp. 337 – 361.
Grosh, M., Leite, P., Wai-Poi, M., & Tesliuc, E. (Eds.). (2022). Revisiting Targeting in Social Assistance: A New Look at Old Dilemmas. World Bank Publications.
Headey, D. & Ruel, M. (2020, April 23). The COVID-19 nutrition crisis: What to expect and how to protect. International Food Policy Research Institute. https://www.ifpri.org/blog/covid-19-nutrition-crisis-what-expect-and-how-protect
Jacob, K., King, P., Mangalagiu, D., & Rodriguez-Labajos, B. (2019). Approach to assessment of policy effectiveness. Global Environment Outlook–GEO-6: Healthy Planet, Healthy People, 272-281.
Jessica, A. (2022, January 27). The 2nd G20 Joint Finance and Health Task Force (JFHTF) Meeting: G20 Finance and Health Ministries Continue to Collaborate on Pandemic and Future Health Emergencies Prevention, Preparedness, and Response (PPR). G20 Information and News. https://g20.org/the-2nd-g20-joint-finance-and-health-task- force-jfhtf-meeting-g20-finance-and-health-ministries-continue-to-collaborates-on- pandemic-and-future-health-emergencies-prevention-preparedness-and-resp/.
Khalid, H., Gill, S., & Fox, A. M. (2019). Global aid for nutrition-specific and nutrition-sensitive interventions and proportion of stunted children across low- and middle-income countries: does aid matter?. Health Policy and Planning, 34 (2019). https://doi.org/10.1093/heapol/czz106.
National Audit Office. (2008). Evaluation of Regulatory Impact Assessments 2006-07 (Publication No HC 606 Session 2006-2007). https://www.nao.org.uk/wp- content/uploads/2007/07/0607606.pdf.
NHS. (n.d.). Malnutrition. Accessed at 7 July 2022. https://www.nhs.uk/conditions/malnutrition/.
Osendarp, S., Akuoku, J. K., Black, R. E., Headey, D., Ruel, M., Scott, N., & Heidkamp, R. (2021). The COVID-19 crisis will exacerbate maternal and child undernutrition and child mortality in low-and middle-income countries. Nature Food, 2(7), 476-484.
Perez-Escamilla, R., Bermudez, O., Buccini, G. S., Kumanyika, S., Lutter, C. K., Monsivais, P., & Victora, C. (2018). Nutrition disparities and the global burden of malnutrition. BMJ, 361. https://doi.org/10.1136/bmj.k2252.
UNICEF. (2020). Child Nutrition and Covid-19 Database July 2020. https://data.unicef.org/topic/nutrition/child-nutrition-and-covid-19/.
USAID. (2022, March 24). Private Sector Collaboration for COVID-19 Vaccine Delivery. GH Supply Chain. https://www.ghsupplychain.org/news/private-sector-collaboration- covid-19-vaccine-delivery.
WHO. (2017). Double-duty actions for nutrition: policy brief. https://www.who.int/publications/i/item/WHO-NMH-NHD-17.2.
World Obesity Federation. (2022). World Obesity Atlas 2022. Retrieved from https://s3-eu- west-1.amazonaws.com/wof-files/World_Obesity_Atlas_2022.pdf.